
The Creatine Blueprint: How Creatine Impacts Athletic Performance
Creatine is the most extensively studied supplement in sports science. With over 500 peer-reviewed studies and decades of consistent evidence (Rawson & Volek, 2003), it stands as one of the most reliable, effective, and safe performance-enhancing compounds available to athletes. And yet, despite its proven track record, its use in baseball and by younger athletes is often plagued by misinformation, half-truths, or outright misuse.
This article aims to correct the narrative and offer a clear, scientifically grounded understanding of creatine, how it works, and how to implement it effectively for long-term performance gains.
What Is Creatine and How Does It Work?

Creatine is a nitrogen-containing compound synthesized endogenously in the human body from three amino acids: arginine, glycine, and methionine. It is produced in the liver, kidneys, and pancreas at a rate of approximately 1 gram per day and is also obtained through the diet, predominantly from red meat (Branch, 2003). The average omnivorous diet provides an additional 1 gram per day, totaling around 2 grams of creatine intake daily. Roughly 95% of this creatine is stored in skeletal muscle, with about two-thirds existing as phosphocreatine (PCr) and the rest as free creatine (Kreider, 2003).
Phosphocreatine serves as a phosphate donor for the rapid resynthesis of adenosine triphosphate (ATP) via the enzyme creatine kinase. ATP is the primary energy currency of muscle contractions, particularly during short-duration, high-intensity activities like pitching, sprinting, or lifting. During such efforts, PCr levels can drop by 30% to 80% depending on the intensity and duration of the activity (McCartney et al., 1986), which directly impacts performance. Replenishing PCr stores between efforts is a critical factor in maintaining output during repeated high-intensity bouts (Alghannam, 2012).
Creatine Supplementation: What the Research Shows
Supplementing with creatine monohydrate increases total muscle creatine content by approximately 20%, reaching a saturation point around 150-160 mmol/kg of dry muscle mass (Greenhaff et al., 1993). This elevation in muscle creatine enhances the ability to perform repeated bouts of high-intensity work, increases lean body mass, and improves strength and muscular endurance. In a meta-analysis of resistance training studies, creatine supplementation led to an average 8% increase in one-repetition maximum (1RM) strength and a 14% improvement in maximal reps (Branch, 2003).
The benefits are especially relevant for anaerobic tasks lasting under 30 seconds. While benefits can extend to activities lasting up to 150 seconds, the evidence is strongest for very short, intense bursts of effort (Balsom et al., 1994). These findings align well with the energy system demands of baseball, particularly in pitching and explosive position-specific movements.
In addition to its energetic role, creatine may exert anabolic effects through mechanisms such as satellite cell proliferation, increased activity of myogenic transcription factors, and enhanced insulin-like growth factor-1 (IGF-1) signaling (Saremi et al., 2010). One study found a direct correlation between changes in intramuscular IGF-1 concentrations and increases in lean mass following creatine use (Burke et al., 2008). These non-energetic effects may help explain the observed hypertrophy benefits beyond mere water retention.
Debunking the Water Weight Myth
A common criticism of creatine is that weight gain is primarily water. It is true that during the initial week of creatine loading, individuals typically gain 1 to 2 kilograms due to increased intracellular water from osmotic shifts (Green et al., 1996). However, long-term studies reveal that continued supplementation leads to genuine increases in fat-free mass and muscle contractile proteins (Volek & Kraemer, 1996). In other words, the gains extend beyond water; they include actual muscle tissue development.
Moreover, creatine does not appear to significantly increase subcutaneous water retention. Most of the fluid is stored intracellularly within muscle tissue, contributing to the "fuller" muscle appearance that many athletes notice.
Proper Dosing and Timing

The standard dosing protocol begins with a 5-7 day loading phase, where athletes consume 20-25 grams of creatine per day, divided into 3-4 doses to minimize gastrointestinal side effects (Poortmans & Francaux, 2000). Following the loading phase, a maintenance dose of 3-5 grams per day is sufficient to maintain muscle saturation. When dosing based on body weight, the standard recommendation is 0.3 g/kg/day during loading and 0.03 g/kg/day for maintenance.
It is important to note that loading is not strictly necessary. Daily supplementation without a loading phase will eventually lead to the same saturation levels, but it will take approximately three to four weeks to reach peak muscle creatine stores (Greenhaff et al., 1994).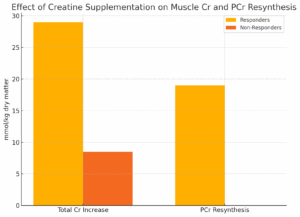
Several studies have explored the effect of timing. While creatine does not exert acute ergogenic effects like caffeine, taking it post-workout appears to offer a slight edge. One study found that participants who took creatine after training gained more lean mass than those who took it beforehand (Antonio & Ciccone, 2013), although the results did not reach statistical significance. Given the low cost and ease of implementation, post-workout dosing with a carbohydrate- or protein-containing meal is generally recommended.
Creatine and Carbohydrate Synergy
Creatine uptake is enhanced in the presence of insulin. Studies have demonstrated that pairing creatine with 90-100g of simple carbohydrates increases muscle creatine retention by up to 60% compared to creatine alone (Green et al., 1996). Another study showed that creatine retention increased by 25% when consumed with a meal containing both carbohydrates and protein (Steenge et al., 2000).
While these enhanced uptake rates may not always translate into greater performance outcomes (Theodorou et al., 2005), the practice of taking creatine with a post-workout meal is still considered optimal—especially during the initial saturation phase.
Who Responds to Creatine—and Who Doesn’t?
Approximately 20-30% of individuals are classified as "non-responders" to creatine (Syrotuik & Bell, 2004). These individuals typically have higher baseline muscle creatine levels and a lower proportion of Type II muscle fibers, both of which limit the degree of further creatine storage and performance enhancement. Diet is also a factor: people with high red meat intake may already have near-maximal creatine stores, reducing the impact of supplementation (Tarnopolsky, 2010).
By contrast, vegetarians tend to respond more dramatically to creatine. Studies show that vegetarians gain more lean mass (Burke et al., 2003) and demonstrate greater cognitive performance improvements with supplementation (Rae et al., 2003), likely due to lower baseline creatine levels.
Cognitive and Neuroprotective Benefits
Although most known for its role in sports performance, creatine also supports brain function. The brain uses creatine as a rapid energy source during high-demand cognitive tasks. Clinical trials have found improvements in working memory, processing speed, and long-term memory in both young and older adults (Benton & Donohoe, 2011; Rawson & Venezia, 2011). There is even early research suggesting neuroprotective effects in conditions like Parkinson’s disease and traumatic brain injury (Beal, 2011).
These cognitive benefits appear to be amplified in vegetarians, likely due to lower baseline tissue creatine stores (Yazigi Solis et al., 2014).
Forms of Creatine and Supplement Quality
Despite aggressive marketing, creatine monohydrate remains the gold standard. It is the most studied, the most effective, and the most cost-efficient form available (Kreider, 2003). Other forms—such as creatine ethyl ester, citrate, or nitrate—have failed to demonstrate superiority and are often less stable or more expensive (Spillane et al., 2009).
To ensure purity, athletes are advised to use creatine products certified by third-party testers like Creapure or Labdoor (Greenwood et al., 2003).
Creatine Safety: What the Science Says
Creatine has been scrutinized for decades, and the consensus is clear: it is safe for healthy individuals (Poortmans & Francaux, 2000; Kim et al., 2011). The most common concern is kidney damage, based on elevated serum creatinine levels. However, this biomarker merely reflects increased turnover and is not indicative of renal stress in healthy individuals (Schilling et al., 2001).
Long-term studies—some lasting 4 to 5 years—have shown no adverse health effects from creatine supplementation (Antonio et al., 2008). The only documented risks are in individuals with pre-existing kidney conditions or those taking nephrotoxic medications.
There is some speculation around creatine’s impact on hair loss due to its association with elevated DHT levels. One study found a 50% increase in DHT after 3 weeks of creatine supplementation (van der Merwe et al., 2009). While the data is limited and the effect not definitively linked to hair loss, those with a genetic predisposition to male pattern baldness may want to monitor their response.
Conclusion: Creatine in Context
Creatine is not a miracle supplement—it’s a scientifically validated tool. Its effectiveness is maximized when integrated into a comprehensive program that includes resistance training, whole-food nutrition, and proper recovery protocols. For baseball athletes, where high-intensity bursts, recovery, and long-term development matter, creatine offers meaningful benefits when used correctly.
At TopVelocity, our philosophy is clear: tools don’t build athletes—systems do. We integrate creatine supplementation only after the foundational pillars of performance are in place.
If you're ready to implement creatine the right way—backed by decades of science and real-world application—schedule a free consultation with Dr. Pat McNeil.

References
-
Rawson, E.S., & Volek, J.S. (2003). Effects of creatine supplementation and resistance training on muscle strength and weightlifting performance. Journal of Strength and Conditioning Research, 17(4), 822-831.
-
Branch, J.D. (2003). Effect of creatine supplementation on body composition and performance: a meta-analysis. International Journal of Sport Nutrition and Exercise Metabolism, 13(2), 198–226.
-
Kreider, R.B. (2003). Effects of creatine supplementation on performance and training adaptations. Molecular and Cellular Biochemistry, 244(1–2), 89–94.
-
McCartney, N., et al. (1986). Muscle power and metabolism in maximal intermittent exercise. Journal of Applied Physiology, 60(4), 1164–1169.
-
Alghannam, A.F. (2012). Metabolic Limitations of Performance and Fatigue in Football. Asian Journal of Sports Medicine, 3(2), 65–73.
-
Greenhaff, P.L., et al. (1993). Influence of oral creatine supplementation on muscle torque during repeated bouts of maximal voluntary exercise. Clinical Science, 84(5), 565–571.
-
Balsom, P.D., et al. (1994). Creatine in humans with special reference to creatine supplementation. Sports Medicine, 18(4), 268–280.
-
Saremi, A., et al. (2010). Effects of oral creatine and resistance training on serum myostatin and GASP-1. Molecular and Cellular Endocrinology, 317(1-2), 25–30.
-
Burke, D.G., et al. (2008). Effect of creatine supplementation and resistance-exercise training on muscle insulin-like growth factor in young adults. International Journal of Sport Nutrition and Exercise Metabolism, 18(4), 389–398.
-
Green, A.L., et al. (1996). Carbohydrate ingestion augments skeletal muscle creatine accumulation during creatine supplementation in humans. American Journal of Physiology, 271(5 Pt 1), E821–E826.
-
Volek, J.S., & Kraemer, W.J. (1996). Creatine supplementation: its effects on human muscular performance and body composition. Journal of Strength and Conditioning Research, 10(3), 200–210.
-
Poortmans, J.R., & Francaux, M. (2000). Adverse effects of creatine supplementation: fact or fiction? Sports Medicine, 30(3), 155–170.
-
Greenhaff, P.L., et al. (1994).
-
Antonio, J., & Ciccone, V. (2013). The effects of pre versus post workout supplementation of creatine monohydrate on body composition and strength. Journal of the International Society of Sports Nutrition, 10:36.
-
Steenge, G.R., et al. (2000). Protein- and carbohydrate-induced augmentation of whole body creatine retention in humans. Journal of Applied Physiology, 89(3), 1165–1171.
-
Theodorou, A.S., et al. (2005). Effects of acute creatine loading with or without carbohydrate on repeated bouts of maximal swimming in high-performance swimmers. Journal of Strength and Conditioning Research, 19(2), 265–269.
-
Syrotuik, D.G., & Bell, G.J. (2004). Acute creatine monohydrate supplementation: a descriptive physiological profile of responders vs. nonresponders. Journal of Strength and Conditioning Research, 18(3), 610–617.
-
Tarnopolsky, M.A. (2010). Caffeine and creatine use in sport. Annals of Nutrition and Metabolism, 57(Suppl 2), 1–8.
-
Burke, D.G., et al. (2003). Effect of creatine and weight training on muscle creatine and performance in vegetarians. Medicine & Science in Sports & Exercise, 35(11), 1946–1955.
-
Rae, C., et al. (2003). Oral creatine monohydrate supplementation improves brain performance: a double-blind, placebo-controlled, cross-over trial. Proceedings of the Royal Society B: Biological Sciences, 270(1529), 2147–2150.
-
Benton, D., & Donohoe, R. (2011). The influence of creatine supplementation on the cognitive functioning of vegetarians and omnivores. British Journal of Nutrition, 105(7), 1100–1105.
-
Rawson, E.S., & Venezia, A.C. (2011). Use of creatine in the elderly and evidence for effects on cognitive function in young and old. Amino Acids, 40(5), 1349–1362.
-
Beal, M.F. (2011). Neuroprotective effects of creatine. Amino Acids, 40(5), 1305–1313.
-
Yazigi Solis, M., et al. (2014). Brain creatine depletion in vegetarians? A cross-sectional 1H-magnetic resonance spectroscopy (1H-MRS) study. British Journal of Nutrition, 111(7), 1272–1274.
-
Spillane, M., et al. (2009). The effects of creatine ethyl ester supplementation combined with heavy resistance training. Journal of the International Society of Sports Nutrition, 6:6.
-
Greenwood, M., et al. (2003). Differences in creatine retention among three nutritional formulations of oral creatine supplements. Journal of Exercise Physiology Online, 6(3), 37–43.
-
Kim, H.J., et al. (2011). Studies on the safety of creatine supplementation. Amino Acids, 40(5), 1409–1418.
-
Schilling, B.K., et al. (2001). Creatine supplementation and health variables: a retrospective study. Medicine & Science in Sports & Exercise, 33(2), 183–188.
-
Antonio, J., et al. (2008). Long-term creatine supplementation and liver/kidney functions in collegiate football players. International Journal of Sport Nutrition and Exercise Metabolism, 18(4), 397–407.
-
van der Merwe, J., et al. (2009). Creatine supplementation affects DHT: testosterone ratio. Clinical Journal of Sport Medicine, 19(5), 399–404.

