
With injuries to pitchers costing major league baseball teams more than $420 million a year, you can imagine that injury prevention is a huge part of the day-to-day operation for most teams. The injury that we keep hearing about is a UCL tear requiring “Tommy John” surgery, but another injury is lurking: Thoracic Outlet Syndrome. “Dead arm” is the term we think of most often but the medical term is Thoracic Outlet Syndrome. Symptoms are arms that feel weak, cold, tingling, or some pitchers just say that their arm feels dead. Baseball players can be at an increased risk of this condition because of the mechanical strain that repetitive overhead throwing puts on the body. The goal of this soapbox is to educate you on the condition of Thoracic Outlet Syndrome, to identify areas of the body that are at risk, and to provide some basic maintenance exercises to prevent the issue or help with some of the symptoms you may be already having.
*Disclaimer* If you are having vascular symptoms i.e coldness, swelling, or changes in the color of your arm, get medical advice immediately to rule out something serious like an Aneurysm or Thrombosis.
What is Thoracic Outlet Syndrome?
Thoracic Outlet Syndrome is a condition that involves the compression of the nerves and/or blood vessels running through the cervicothoracobrachial region (from your neck to the arm). The most common form is the neurological condition which occurs in 95% of all Thoracic Outlet Syndrome cases and can involve symptoms like muscle atrophy or numbness and tingling in the arm. Misdiagnosis is common because the pain pattern resembles other injuries in the shoulder girdle like a rotator cuff or biceps tendinosis. The second form of Thoracic Outlet Syndrome is vascular and occurs when the arteries/veins running underneath the clavicle and the axillary region become compressed, leading to swelling, change in skin color, and temperature changes in the arm.
Where can Thoracic Outlet Syndrome Occur?
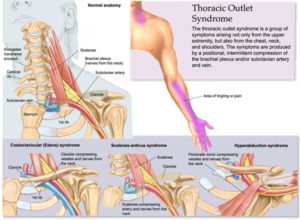 Three areas are identified with Thoracic Outlet Syndrome. The first is between the anterior and middle scalene muscles, known as the inter scalene triangle. Nerves run through these two muscles, underneath the clavicle (collarbone), and into the axillary (armpit) region. The second location is between the clavicle and the first rib, known as the costoclavicular space. Multiple factors can contribute to compression in this region. One is that the scalenes, which attach to the first rib, tighten and pull up on that rib, decreasing the space for the nerves and vessels. A similar thing happens when the shoulder girdle is being pulled down or tipped forward as with tight lats, a tight subclavius muscle or, more importantly, a tight or hypertrophied pec minor. This leads to the third location which is underneath the pec minor in the subcoracoid tunnel. This is a particular area of concern because of the stress placed in the region while the arm is in an abducted and externally rotated position! Sound familiar? This is the position your arm is in whenever you are in the late cocking phase of throwing. Repetitive demands on the shoulder, such as throwing, can lead to adaptive changes: increased external rotation, anterior capsule laxity, and posterior capsule tightness. All of these adaptations can result in increased pressure on the front of the shoulder which can compress the arterial blood supply.
Three areas are identified with Thoracic Outlet Syndrome. The first is between the anterior and middle scalene muscles, known as the inter scalene triangle. Nerves run through these two muscles, underneath the clavicle (collarbone), and into the axillary (armpit) region. The second location is between the clavicle and the first rib, known as the costoclavicular space. Multiple factors can contribute to compression in this region. One is that the scalenes, which attach to the first rib, tighten and pull up on that rib, decreasing the space for the nerves and vessels. A similar thing happens when the shoulder girdle is being pulled down or tipped forward as with tight lats, a tight subclavius muscle or, more importantly, a tight or hypertrophied pec minor. This leads to the third location which is underneath the pec minor in the subcoracoid tunnel. This is a particular area of concern because of the stress placed in the region while the arm is in an abducted and externally rotated position! Sound familiar? This is the position your arm is in whenever you are in the late cocking phase of throwing. Repetitive demands on the shoulder, such as throwing, can lead to adaptive changes: increased external rotation, anterior capsule laxity, and posterior capsule tightness. All of these adaptations can result in increased pressure on the front of the shoulder which can compress the arterial blood supply.
How can we attack Thoracic Outlet Syndrome?
Outside of God-given anatomic anomalies, like an additional cervical rib or altered attachment of the muscles and ligaments, we can adapt the tissue, improve posture, and promote proper throwing mechanics to minimize the stress placed on all structures. As stated before, if you have had vascular symptoms for an extended time, let your personal or team doctor know. Don’t hope it will just go away! For those who think they may have had some slight symptoms or just want to try and prevent possible future injury, then the following should be helpful.
Starting with the scalenes: As these muscles tighten, they pull on the first rib. These are accessory respiratory muscles, meaning they should help the diaphragm expand the rib cage while we breathe. If you have a bad habit of not efficiently using the Diaphragm, then these muscles get overworked and will hypertrophy, which can mean bad news. Another reason these muscles get shortened is the player’s posture. If you stand with your head forward and your shoulders rounded, then these muscles will shorten. This becomes a problem when you really need to expand the body to achieve an efficient throwing pattern. Imagine how much strain gets placed in this region of your neck as your lats, scapular stabilizers, and internal rotators pull the shoulder girdle down while your trunk tilts forward and rotates during the acceleration and follow-through phase of pitching. Below is a video of how to release the scalenes, mobilize the first rib, and a couple of my favorite posture exercises.
The next region to consider is the pectoral and axillary region. Tissue in this region can restrict chest expansion and create an increased risk of compression along the anterior portion of the shoulder. Some of the main contributors include the Clavipectoral Fascia and the Pectoralis Minor muscle. I stressed the importance of the pec minor earlier and I’ll do it again. If this muscle is tight or shortened, it tilts the scapula forward, makes the scapula rotate downward, and promotes adduction of the shoulder which is a BIG problem for an overhead athlete trying to get into a throwing position. Below is a video on how to release/stretch this muscle and expand the fascial system throughout the pectoral region.
The final area I want to touch on is an area of universal concern for not only Thoracic Outlet Syndrome but all upper extremity injuries: scapular stability. If the scapula is not maintained in a stable position throughout the throwing cycle, due to fatigue, muscle weakness, or capsular tightness, players are at risk of injury. I want to touch on two muscles that typically get weak: the Serratus Anterior and the Lower Trapezius. These muscles help posteriorly tilt the scapula while providing an upward rotational force to allow for appropriate positioning of the humeral head. If they are weak and the scapula is allowed to tip forward, then it strains/compresses the anterior tissue of the shoulder. If you combine this weakness with a tight posterior capsule, common in baseball players due to the required muscle strength to decelerate the arm, then the shoulder is at even greater risk. Below is a video with exercises to assist scapular stabilization, upward rotation, and posterior tilting.
I hope this has been helpful and please realize that this is just a small piece of the pie. Overhead lifting and The Throwers Ten and Advanced Throwers Ten are great programs to strengthen and stabilize the shoulder, but you shouldn’t stop there. If you don’t have the strength and stability in the core and lower half, then the body will compensate to find power elsewhere. Do yourself a favor and train to become a great athlete, not just a pitcher, with the 3X Pitching Velocity program.


I have TOS. I developed a 8 inch long blood clot in my left arm.
After 2 years on blood thinners the blood clot has almost completely dissolved.
I have seen several specialist and had many tests including ultrasound.
The diagnosis is, I have a very restricted space in my thoracic area and I put repeated pressure on my subclavian vein When I raise my arm resulting in a thrombosis.
The doctors advice, moving forward, is to not raise my arms, stop all sports and physical activities that involves raising the arms. I do not have an extra rib. This TOS came on when I was 55 and I’d had never experience issues in the past. I feel the restrictions in my thoracic area must be caused by muscle constriction and I would expect I could reverse the issue by stretching the muscles out again.
Unfortunately when I ask the specialist( a vascular surgeon) about physiotherapy, he says no and that I could actually cause more trauma to the area during physiotherapy.
I am very frustrated,.
Can Someone help me?
I? have an extra rib and it ended my baseball career. The pain I experienced was unbearable and finished my career